
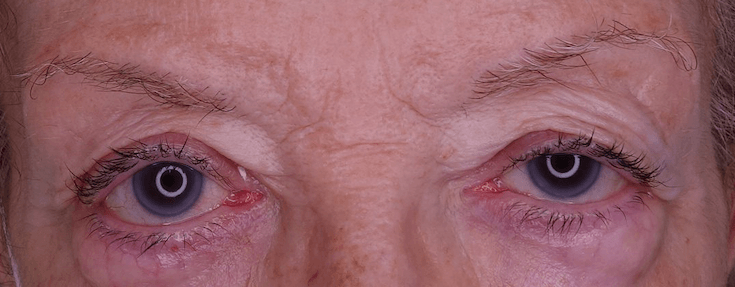
Palpebral ptosis is the dropping of the upper eyelid and is one of the most common oculoplastic problems. This anomalous position of the eyelid is usually caused by a dysfunction of the lifting muscle, either by degenerative or congenital causes, and can affect both adults and children. In the most serious cases, it can affect the visual axis by blocking the pupil and limiting or even totally preventing vision. The treatment of palpebral ptosis allows to improve the vision field by raising the eyelid again while improving the physical appearance of the affected person by improving the look.
Ptosis in children can be congenital, that is, the patient may have been born with this problem, or it can be acquired, more frequently in adults, and be caused due to aging tissues, lack of nerve stimulation in the muscle, the appearance of a cyst or tumor, or poor function of the muscle that raises the eyelid. The main cause of palpebral ptosis is the passage of time.
Symptoms of palpebral ptosis can vary according to the severity of the disease, although they are usually:
It is important to pay attention to these symptoms, especially in the most subtile ones, since if they are not treated, they can lead to lazy eye or ambylopia, due to vision deprivation. Also, babies with palpebral ptosis should visit an ophthalmologist as soon as possible to evaluate the affectation and the most appropriate treatment.
Palpebral ptosis is usually due to a dysfunction of the upper eyelid elevator muscle, which can be caused by a number of factors. Thus, according to the origin of this dysfunction can be classified in different types of ptosis:
Choosing the most appropriate treatment in each case will depend on the cause of the ptosis and above all on the severity of the vision impairment, although in most cases it usually involves surgical correction. Depending on the level of muscle function, the oculoplastic surgeon will choose one technique or another.
If the loss of function of the elevator muscle is slight or moderate, a partial resection (shortening) of the muscle is usually chosen, either by anterior via (incision outside the eyelid) or posterior via (incision on the inside of the eyelid, the tarsal conjunctiva). In critical cases, it will be opted to create elements of eyelid suspension, substitutes for the ineffective muscle, which will help in the elevation of the eyelid. In any case, the final objective is always to elevate the upper eyelid to its normal position, to improve the symmetry of the two eyelids and to recover the visual field. It is of vital importance to preserve the eyeball and ensure that after surgery the eyelid closes completely, so the knowledge of the palpebral anatomy of your oculoplastic surgeon will make your eye as protected as possible.
In the case of children with amblyopia or lazy eye, ptosis correction surgery can be accompanied by other complementary treatments, such as correction through eye patches, glasses or drops to strengthen the weakest eye.
The droopy eyelid operation is performed under local anesthesia and sedation and on an ambulatory basis, except in young children, who are operated under general anesthesia. It is usually realized with little visible incisions and with minimally invasive techniques, always looking for the best possible aesthetic result.

Congenital ptosis is that ptosis that the patient suffers since birth. It is usually hereditary and is related to an improper development of the lifting muscle. In 75 % of the cases it affects only one eyelid.
In some cases, such as simple congenital ptosis, it is possible to initially try treatments to correct the amblyopia. If these do not improve the ptosis, surgical correction will be used.
Surgery to correct palpebral ptosis is usually performed with incisions in the skin flanks, which makes the scars hardly visible, and with minimally invasive techniques, always looking for the best possible aesthetic result.
It is usually quite fast, hygienic measures are recommended on the wound, application of local cold and moisturizing treatment to preserve the eye. The bruises that usually emerge leave between the first and third week of the postoperative period.
Usually a visit is made the day after the operation. Another review is made a week in which they can remove the sutures and then another visit a month after the operation in which they will be the release of the operation.
The accumulated fatigue during the day can worsen the fall of the eyelid and magnify the asymmetry between one eyelid and another. With rest it usually returns to the previous situation. Alcohol can also cause this temporary worsening.
The oculoplastic surgeon is an ophthalmologist specialized in eyelids, who knows the palpebral anatomy and takes special care of the eye to preserve its protective function of the ocular surface.
Superior blepharoplasty is responsible for removing excess redundant skin from the upper eyelid without modifying the palpebral opening, while the purpose of palpebral ptosis surgery is to increase the opening of the eyelid in order to see better. Both techniques can be associated at the same time, always previously evaluated by your oculoplastic surgeon.
Lagophthalmos is the difficulty of closing the eyelid with the blink, which leads to a higher risk of exposure of the eye to irritation, just the opposite of what occurs in palpebral ptosis in which the eyelid falls more and has no problem in the palpebral closure.
Pseudoptosis is the false appearance of eyelid dropping without the palpebral opening being altered, which is affected in the palpebral ptosis. Pseudoptosis can be produced by an optical effect produced by the variation of the position of the eyelid folds or by an excess of skin in the upper eyelid that causes a false sensation of having the eyelid drooping.


Blepharitis is an inflammation that occurs at the edge of the eyelids causing redness, peeling and swelling of the eyelids. It is usually chronic but it does not usually cause permanent damage.

Blepharoplasty is a minimally invasive operation that removes excess skin, and sometimes fat, from the eyelids. With this surgery it is possible to improve the tired aspect of the face.

Eyelid malpositions are defects in eyelid position that usually appear later in life. An eyelid rolled inward leads to an entropion, while an eyelid rolled outward causes an ectropion.
Contact us or request an appointment with our medical team.


 Request an appointment
Request an appointment